Non-carious loss of tooth structure is a problem that is often found in senior citizens and is a cause of many complaints. It is not a new entity but has acquired more attention in recent time.
National Board of Examinations in Medical Sciences have declared the dates for NEET MDS, NEET PG & other exams. Candidates can check the exam dates below.
NEET-MDS 2023: January 8, 2023
DNB/DrNB Final Practical Examination – June 2022: October/November 2022
Foreign Medical Graduate Examination (FMGE) December 2022, Foreign Dental Screening Test (FDST) 2022: December 4, 2022
Formative Assessment Test (FAT) 2022: December 10, 2022
DNB/DrNB Final Theory Examination – December 2022: December 21, 22, 23 and 24, 2022
Fellowship Entrance Test (FET) 2022: January 20, 2023
FNB Exit Examination 2022: February/March 2023
DNB/DrNB Final Practical Examination – December 2022: Feb/March/April 2023
NEET-PG 2023: March 5, 2023
Distribution of subject wise questions in NEET MDS examination.
The candidates are being advised to check the details and the updated information at the NBE website - https://natboard.edu.in/ as the dates mentioned are tentative and subject to approval and confirmation.
In earlier articles on radiography, you studied the effects of ionizing radiation on biological tissues. These effects can be divided into two types- Deterministic and Stochastic. Therefore, the radiation safety becomes of paramount importance white taking a radiograph.
In this article termed as radiation physics, we shall talk about the ways, the x-rays are produced, the events that occur at atomic level during their production and how can one save oneself and others.
Production of X Rays
Electrons that travel from the filament to the tungsten convert part of their kinetic energy into x-ray photons. This phenomenon occurs by the formation of bremsstrahlung and characteristic radiation.
Radiation biology is the study of effects of ionizing radiation on living systems. In this article we shall talk about the harmful effects of ionizing radiation on tissues, how does it occur, and how sensitive different types of cells are?
A cyst is defined as “an epithelial lined pathologic cavity”. The periapical/radicular cyst is an odontogenic cyst. The classification of the cysts can be seen HERE. It is important to read for ADC Exams or NEET MDS purpose.
Periapical/Radicular cyst
Periapical cysts are inflammatory cysts. Their epithelial lining originates from the odontogenic epithelium of the tooth buds that remains within periodontal ligaments (epithelial rests of Malassez) after completion of tooth maturation. Due to inflammatory response, the epithelial rests of Malassez start proliferating and provide cystic lining.
Dentigerous (Follicular) Cysts are the second most commonly occurring odontogenic cysts after periapical cyst and the most common developmental cysts of the jaws. By definition, a dentigerous cyst is attached to the tooth cervix (enamel-cementum junction) and encloses the crown of the unerupted tooth.
Photograph1: Dentigerous cyst surrounding the crown of right mandibular third molar and going upward in ascending ramus. [1]
Etiology and Pathogenesis of Dentigerous Cyst
A dentigerous cyst originates from the enamel organ remnant or reduced enamel epithelium. The expansion of the dentigerous cyst is related to epithelial proliferation, release of bone-resorbing factors, and an increase in cyst fluid osmolality.
Clinical Features of Dentigerous Cyst
Dentigerous cysts are most commonly seen associated with third molars and maxillary Canines. The peak incidence of dentigerous cysts occurs between twenty to 40 years. Males have more predilection with a ratio of l.6 to 1.
Dentigerous cysts are generally symptomless. The delayed eruption is the most common indication of dentigerous cyst formation. This cyst can achieve significant size, occasionally causes cortical bone expansion but rarely reaches a size that predisposes the patient to a pathologic fracture.
Radiographically, a dentigerous cyst manifests as a well-defined, unilocular or sometimes multilocular radiolucency with corticated margins in attached with the crown of an unerupted tooth. The concerned unerupted tooth is mostly displaced. In the mandible the related radiolucency may extend superiorly from the third molar site into the ramus or anteriorly and inferiorly along the body of the mandible. In maxillary dentigerous cysts in the canine region, extension into the maxillary sinus or to the orbital floor may be seen.
Histopathology.
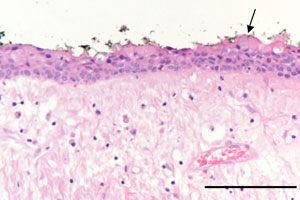
The cyst is lined by stratified squamous epithelium. In a noninflamed dentigerous cyst the epithelial lining is nonkeratinized. It remains approximately four to six cell layers thick. Sometimes, numerous mucous cells, ciliated cells, and rarely, sebaceous cells may be found in the lining of the epithelium. The epithelium-connective tissue junction is generally flat. But when secondary inflammation established, epithelial hyperplasia may be noted.
Photomicrography 2: showed a thin non-keratinized epithelial lining composed of 2–3 layers of cuboidal epithelial cells and a fibrous connective-tissue wall loosely arranged. The arrow indicates an occasional mucous cell (bar = 0.2 mm) [1]
Differential diagnosis
When it is small, it is difficult to differentiate a dentigerous cyst from a large but normal dental follicle. When larger, the differential is essential that of lytic lesions of the jaw and includes:
periapical cyst
aneurysmal bone cyst
ameloblastoma
odontogenic keratocyst
fibrous dysplasia
Stafne cyst
Treatment
Removal of the associated tooth and enucleation of the soft tissue part is definitive therapy in most cases. When cysts affect significant portions of the mandible, exteriorization or marsupialization of the cyst is done to allow for decompression and subsequent shrinkage of the lesion followed by surgical enucleation.
Odontogenic keratocyst (OKC) is a parakeratin lined cyst like lesion within bone.
OKCs mostly occur in the 2nd and 3rd decades of life; although can occur over a wide age range with male predilection. Odontogenic keratocyst comprises of 4 to 12 percent of all odontogenic cysts. Ninety percent of odontogenic keratocysts are solitary. Multiple cysts are found in Nevoid Basal Cell Carcinoma Syndrome / Gorlin Syndrome[1].
The most commonly involved body part in mandible, 65-85%; mostly posterior mandible. Normally, they are associated with third molars but may be present without associating with third molars; rarely occur in soft tissues.
They are considered to arise from dental lamina.
Clinical Features
Odontogenic keratocysts are often asymptomatic. They are incidentally discovered on radiographs. They can cause symptomatic swelling. They can cause parasthesia of lip and teeth. Symptoms of pain and drainage are found if secondarily infected. They can cause local bone and soft tissue destruction, but usually spare teeth and roots.
Swelling observed at the right buccal mucosa (dotted area) posterior to the orifice of Stensen’s duct-arrow head [3].
Odontogenic keratocyst-exposed anterior to the masseter muscle.
Radiographic features
Mostly, they are seen as small unilocular radiolucent lesions with variable sclerotic margins. Larger lesions are often seen multilocular with variable scalloped margins. Therefore, They may resemble radicular cyst, dentigerous cyst, lateral periodontal cyst, and ameloblastoma.
Keratocystic Odontogenic tumer in orthopantomograph being shown as multiple radiolucencies associated with mandibular anterior region, maxillary right and left as well as mandibular left impacted third molar tooth [5].
Classic look to a keratocyctic odontogenic tumor in the right mandible in the place of a former wisdom tooth. Unicystic lesion growing along the bone. Lesion was seen by oral surgeon on routine panoramic radiography without any symptoms [2].
Histology
Histological findings in the above slides are a: The cyst wall is lined with parakeratinized squamous cells with a corrugated surface. b: Nuclei of the cells in the basal layer are palisaded. The rete ridge of the epithelium is not evident [3].
Differential Diagnosis
Ameloblastoma
Dentigerous cyst
Peri-apical cyst
Lateral periodontal cyst
Prognosis
Recurrence rates of OKC are from 20% to 56% with enucleation alone. Resection have been reported to have no recurrences, but it may be considered excessive for a benign cyst.
Multiple lesions can occur when OKCs are associated with Nevoid Basal Cell Carcinoma Syndrome (NBCCS)/Gorlin Syndrome Therefore, early diagnosis and follow-up of the patient with OKC is important as there is always a possibility of developing other features of NBCCS in the future.
Treatment
Treatment is given taking into consideration of recurrence and morbidity. Following are the treatments given alone or in combination to a patient of odontogenic Keratocyst.
Decompression.
Enucleation with possible curettage.
Chemical curettage with Carnoy’s solution.
Marsupialization.
Resection.
Case Studies
For further studies on case reports, you can consult the reference number 4 and 5.
Ref:
Morrison A. Odontogenic keratocyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillakeratocyst.html. Accessed September 11th, 2022.
K. M. Veena, Rekha Rao, H. Jagadishchandra, Prasanna Kumar Rao, "Odontogenic Keratocyst Looks Can Be Deceptive, Causing Endodontic Misdiagnosis", Case Reports in Pathology, vol. 2011, Article ID 159501, 3 pages, 2011. https://doi.org/10.1155/2011/159501