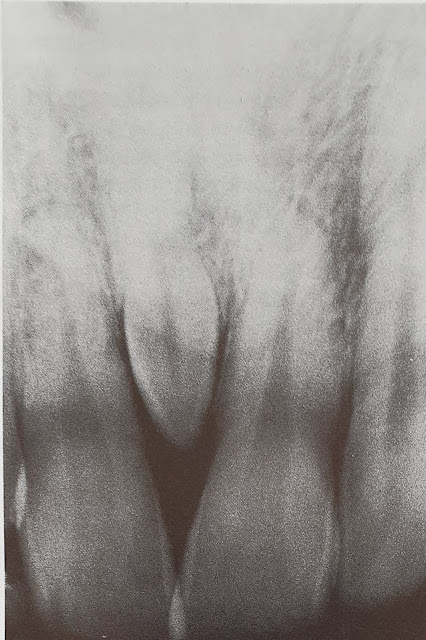
Dens invaginatus, dens in dente or tooth with in a tooth is a rare developmental anomaly. In it, the lingual pit is extended deep in to the crown or root, in later instance causing pulpitis. It is mostly seen in the maxillary lateral incisors but may be found in any anterior tooth.
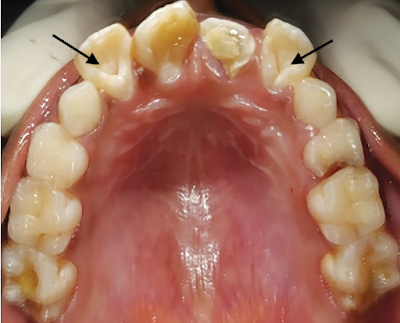 |
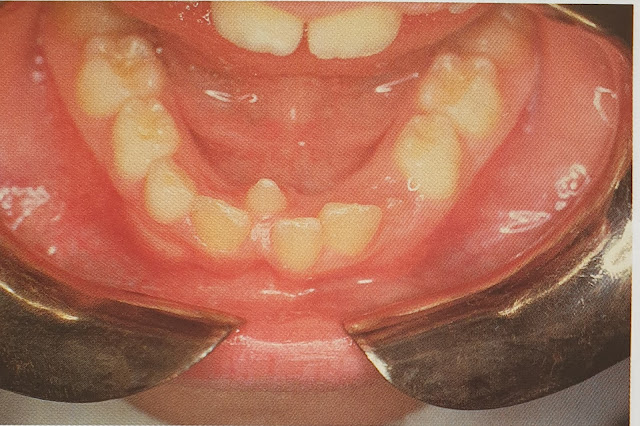
| Dens in Dente-lateral incisors |
The cause of dens in dente in not known but role of genetic factor can not be established. In early stage, it can be treated by filling or endodontic treatment, if pulp is involved.
 |
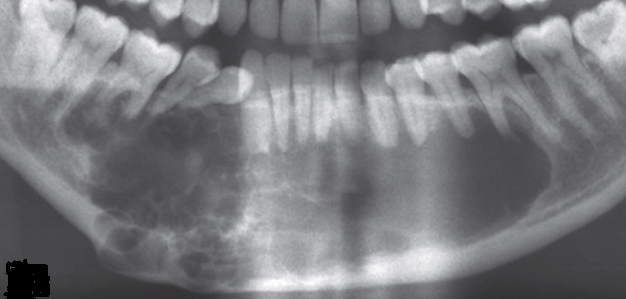
| A. showing Type I Dens Invaginatus in lateral incisors. Note- periapical cyst. B. Type II dens invaginatus in second premolar and C. Type III dens invaginatus in mandibular canine. [1] Ref:
|