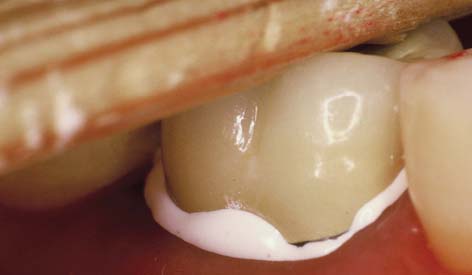
A ceramic crown being placed over a tooth. The excess cement is protruding at margin [1].
The placement of crown is an important step in the longevity of the crown and the comfort of the patient. There are certain points that should be taken into consideration by a dentist during placement i.e. cementation.
The gingival margins should not be inflamed at the time of crown cementation. This may happen due to gingivoplasty or crown lengthening. For a common man, it means, the gum margins of the tooth receiving the artificial crown should not have redness, swelling or puffiness. If there is any, better to wait till it subsides.
The choice of cement/luting agent should be decided based on the type and material of the crown. The available materials are Zinc phosphate, Glass ionomer, Polycarbonate, Zinc silicophosphate, and resin luting agents. The anterior crowns need different cementing material than that of posterior crowns. The all ceramic crowns are best cemented by resin luting agents, but the use is limited to the cementation of anterior crowns. The reason is, after cementation, it becomes extremely difficult to remove set resin from the interproximal area of posterior teeth. Rest luting materials are brittle enough to break and remove, therefore, they can be used in all areas-anterior as well as posterior.