Ameloblastoma is a rare head and neck tumor with an estimated annual incidence of 0.5 per million population. They constitute 1% of tumors and cysts involving the jaws and accounts for approximately 10% of the odontogenic tumors. Ameloblastomas are originated from the epithelial lining of odontogenic cysts, enamel organ or dental lamina, stratified epithelium of oral cavity or displaced epithelial remnants. They are primarily seen in adults during the third and fourth decade of life with no gender preference and more frequently located in the mandible (80%), especially in the angle and ascending ramus [1].
Even though they are benign and slow-growing lesions, ameloblastomas exhibit locally destructive behavior with a high recurrence rate. Thus, most relapses (50% and even over 80%) occur during the first 5 years after the primary surgery. The major contributing factor for recurrence seems to be the inadequate initial surgical procedure rather than the histological type [1].
Radiographic Features
Radiographically, ameloblastoma typically forms round, cyst-like, radiolucent area with well-defined margins. The smallest lesions appear unilocular; whereas larger ameloblastoma may comprise a few large clustered cysts, giving 'soap-bubble’ or 'multilocular appearance' or ‘honeycomb’ appearance (Fig 1) Expansion of the lesion may be on both, lingual and buccal side.
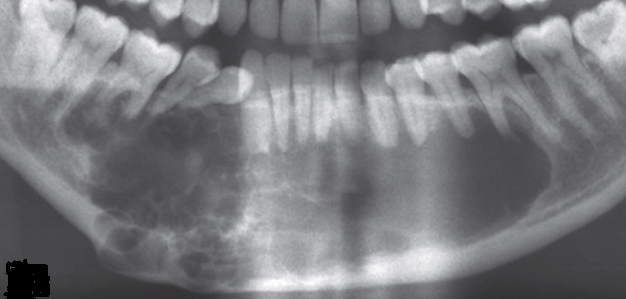 |
| Fig. 1. Ameloblastoma: multilocular appearance |
Differential Diagnosis
Other multilocular lesions that may mimic ameloblastoma radiologically include odontogenic keratocyst, giant-cell granuloma and odontogenic myxoma. Ameloblastoma with a single bony cavity simulate many types of cyst and tumour radiographically.
Treatment
The surgical options for ameloblastoma vary from simple enucleation (with or without bony curettage) to radical excision.
Ref:
- Medina A, Velasco Martinez I, McIntyre B, Chandran R. Ameloblastoma: clinical presentation, multidisciplinary management and outcome. Case Reports Plast Surg Hand Surg. 2021;8(1):27-36. Published 2021 Feb 22. doi:10.1080/23320885.2021.1886854