Darsogluteal Intramuscular Injections

Important points to remember about Kaposi Sarcoma
 |
| Kaposi's sarcoma or oral cavity |
 |
| Kaposi's sarcoma of the skin |
Cemento-osseous dysplasia (COD) is a benign fibro-osseous lesion of bone characterized by the replacement of normal bone by fibrous tissue and subsequently followed by its calcification with osseous and cementum-like material. It arises from the fibroblasts of the periodontal ligaments.
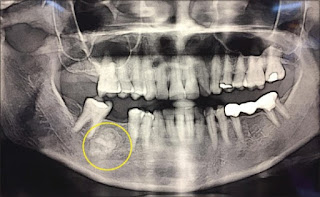 |
| Orthopantamogram showing a well-defined radiopaque mass in the right mandible region extending from the distal root of 45 to the mesial root of 47 [1] |
As per WHO, there are three clinical presentation of cemento-osseous dysplasia.
These occur in the anterior mandible and involve only a few adjacent teeth.
involve few teeth in posterior mandible
The cells of periapical granuloma which are predominantly lymphocytes increase by division at the periphery.
There are hyperaemia and oedema of the PDL; localised increase in the vascularity leads to local bone resorption mediated by osteoclast mediated delayed hypersensitivity. In the specimen slide, cholesterol crystals having needle-like appearance, and eosinic hyaline bodies known as Rushton bodies are seen. Macrophages and multinucleated giant cells are also seen. Epithelium is present.
The cells in the centre are separated from their source of nutrition; hence degenerate and liquefy. This results in an epithelium lined cavity filled with fluid known as periapical cyst.
Treatment involves RCT with apicoectomy or extraction with curettage.
Majority of streptococci produce hyaluronidase, an enzyme that dissolves hyaluronic acid which is a universal intercellular cementing substance. It helps in the spread of infection. Usually staphylococci are good producers of hyaluronidase, so there is no spread of infection and the infection becomes localised in the form of abscess in case of staph infection.